Position statement
Reducing perinatal infection risk in newborns of mothers who received inadequate prenatal care

Posted: Apr 3, 2023 | Updated: Jan 3, 2024
Principal author(s)
Ari Bitnun MD, Laura Sauvé MD, Sergio Fanella MD, Infectious Diseases and Immunization Committee
Abstract
Inadequate prenatal care increases risk for maternal infections going undetected and untreated, putting both the mother’s health and that of her infant at risk. When pregnant women present late to care, routine testing that impacts infant management should include: hepatitis B surface antigen (HBsAg); serology for hepatitis C virus (HCV), human immunodeficiency virus (HIV), and syphilis; and testing for Chlamydia trachomatis and Neisseria gonorrhoeae. If the mother was not tested before or after delivery and is not available for testing, the infant should undergo testing for HIV, HCV, hepatitis B virus (HBV), and syphilis. Testing for C. trachomatis and N. gonorrhoeae should be undertaken if the infant develops compatible clinical manifestations. Rapid turnaround of test results for HIV, HBV, and syphilis is optimal because preventive treatment decisions are time-sensitive. Early and effective preventive interventions are available for newborns at risk for HIV, HBV, syphilis, or gonorrhea. Close clinical follow-up and follow-up testing of infants born to mothers with inadequate prenatal care are warranted, as not all infections can be fully excluded perinatally.
Keywords: Chlamydia; Gonorrhea; Hepatitis B; Hepatitis C; HIV; Newborn; Prenatal care; Syphilis
Background
Lack of or inadequate prenatal care increases the risk of maternal infections being undetected and untreated, putting both the mother’s health and that of her infant at risk. Many correlates of inadequate prenatal care overlap with those associated with higher rates of sexually transmitted infections (STIs), blood-borne infections, and other infections that can be transmitted vertically[1]. In Canada, suboptimal prenatal care impacts historically marginalized (e.g., racialized, Indigenous, and newcomer) populations disproportionately. At the individual level, risk factors for inadequate prenatal care include adolescent pregnancy, high parity, poverty, unemployment, homelessness, imprisonment, substance use disorder, and single parenthood[2]-[12].
This statement provides guidance for the acute care management of newborns of mothers who have received limited or no antenatal care, with the goals of reducing risk for vertical transmission of infections and facilitating early treatment of such infections when they do occur. The primary focus is on infections that are blood-borne or sexually transmitted and for which maternal and infant diagnostic testing is recommended or preventive interventions are available. The statement complements other pathogen- or syndrome-specific Canadian Paediatric Society statements[13]-[17]. The management of maternal infections during pregnancy is beyond the scope of paediatric practice and is not discussed in detail. Nor does this statement address the many issues unrelated to infection that impact the health of infants whose mothers have had limited or no antenatal care.
Pathogens for which routine screening during pregnancy is recommended
Routine prenatal screening recommendations in Canada include testing for hepatitis B virus (HBV), human immunodeficiency virus (HIV), syphilis, Streptococcus agalactiae (Group B streptococcus (GBS)), Chlamydia trachomatis, and Neisseria gonorrhoeae, and confirmation of rubella immunity[18].
Hepatitis B virus
The prevalence of current or past infection with HBV in Canada is approximately 5%, while that of chronic HBV infection (carrier state) is approximately 0.5%[19]. The predominant risk factor for HBV infection is being born to a mother who is a chronic carrier. Other persons at elevated risk include those who inject drugs, household members of chronic carriers, immigrants from endemic regions, and those with risk factors for STIs.
In the absence of preventive interventions, 70% to 90% of mothers who are hepatitis B surface antigen (HBsAg)- and hepatitis B e-antigen (HBeAg)-positive, and 5% to 20% of mothers who are HBsAg-positive but HBeAg-negative, will transmit the virus to their infants, with approximately 90% of infected neonates becoming chronic carriers[20]. The risk of vertical HBV transmission is reduced by approximately 95% through administering HBV vaccine and hepatitis B immune globulin (HBIg) to the newborn within 12 h of birth. In mothers with high viral loads (106 to 108 IU/mL or HBeAg-positive), where the risk of transmission despite vaccine and HBIg is 15% to 30%, administering antiviral medications such as tenofovir or telbivudine during the second and third trimester can significantly reduce transmission risk[20].
Human immunodeficiency virus
With routine screening in pregnancy, maternal treatment with combination antiretroviral therapy (cART) during pregnancy, intrapartum intravenous (IV) zidovudine, infant oral zidovudine, and exclusive formula feeding, the risk of perinatal HIV transmission has been reduced in Canada from 20.2% during the 1990/96 period to 2.9% during the 1997/2010 period, and 1.0% during the 2011/16 period[21][22]. Among mother-infant pairs where the mother started treatment at least 4 weeks before delivery, the risk was 0.2%[21]. Missed opportunities for prevention, observed in the 125 perinatal transmission events between 1997 and 2016, included late maternal diagnosis (intrapartum or postpartum) in approximately 70% of cases, and inadequate maternal treatment despite antenatal diagnosis in approximately 30% of cases[21].
Interventions that may reduce the risk of perinatal transmission in mothers diagnosed with HIV infection late in gestation or intrapartum include immediate initiation of maternal cART, administering IV zidovudine during labour, and Caesarean section if the maternal viral load is ≥1000 copies/mL. Pre-emptive treatment of the infant with cART has been shown to reduce perinatal transmission risk compared with zidovudine monotherapy in untreated mothers diagnosed with HIV infection intrapartum[23].
Treponema pallidum subspecies pallidum (syphilis)
Syphilis is the third most common notifiable STI in Canada after C. trachomatis and N. gonorrhoeae[24]. Syphilis rates have steadily increased since the early 2000s, reaching a rate of 24.7 per 100,000 population in 2020[25]. The highest rate increases have been among persons aged 15 to 39 years[26]. Between 2016 and 2020, syphilis rates in women rose by 740% compared to 70% in men, with women accounting for approximately 30% of overall cases in 2020. Rates of congenital syphilis have also increased substantially, with 103 confirmed cases reported in the 2019/20 period, compared with 20 in the 2016/18 period[26].
The risk of vertical transmission without maternal treatment is approximately 60% to 100% during primary and secondary syphilis, 40% during early latent syphilis, and up to 10% during late latent syphilis[27]. The risk for congenital syphilis is significantly reduced, though not eliminated entirely, with timely antenatal maternal treatment with intramuscular (IM) penicillin[28].
Chlamydia trachomatis
C. trachomatis is the most common STI in Canada, with a reported incidence of 363.2 cases per 100,000 population in 2018[29]. Approximately three-quarters of cases occur in persons 15 to 29 years of age, with incidence rates of 1209.0, 1870.5, and 1024.8 per 100,000 for those aged 15 to 19 years, 20 to 24 years, and 25 to 29 years, respectively[30]. Sixty percent of cases are in women. Among infants born to mothers with untreated active disease, between 30% and 50% will develop clinical conjunctivitis, typically at 2 to 3 weeks post-birth, and 10% to 20% will develop pneumonia, usually between 4 to 8 weeks post-birth[31][32]. Treating the mother antenatally with a single dose of azithromycin 1 gram by mouth (PO) (or with amoxicillin 500 mg 3 times a day for 7 days, or erythromycin 500 mg 4 times a day for 7 days) is highly effective and significantly reduces risk for vertical transmission[18].
Neisseria gonorrhoeae
Between 2009 and 2018, the rate of gonorrhea increased by 190% in Canada, with 56% of cases being in persons aged 15 to 29 years, one-quarter of whom were women[29]. In the absence of maternal treatment or neonatal prophylaxis, the risk of developing gonococcal ophthalmia neonatorum is between 30% and 50% [33][34], with most cases presenting in the first week post-birth with bilateral purulent eye discharge and significant eyelid edema. Other manifestations include scalp abscess and disseminated infection, which can manifest as isolated bacteremia or with focal infections such as arthritis or meningitis. Antenatal treatment with single dose IM ceftriaxone (250 mg) or single dose oral cefixime (800 mg) is highly effective and significantly reduces risk for vertical transmission[18].
Routine application of erythromycin ointment to prevent ophthalmia neonatorum due to N. gonorrhoeae is mandated by law in some Canadian jurisdictions, although the efficacy of this intervention has been questioned[14].
Streptococcus agalactiae (Group B streptococcus)
S. agalactiae (GBS) is a leading cause of neonatal sepsis and focal infections such as pneumonia and meningitis. Intrapartum chemoprophylaxis based on pregnancy screening or risk factors for neonatal disease significantly reduces risk for early onset (0 to 6 days post-birth), but not late onset (≥7 days post-birth) disease in the neonate[16].
Rubella virus
Congenital rubella syndrome is extremely rare in Canada, with all documented cases since 2006 being from women who were infected before arriving in Canada. All women who do not have prior evidence of immunization with a rubella-containing vaccine or who have a non-protective rubella titer on antenatal screening should receive one dose of the MMR vaccine in the immediate post-partum period, preferably before being discharged from hospital.
Pathogens for which screening of mothers or infants should be considered selectively
Routine prenatal care allows for the assessment of many infections that are not routinely screened for but can be transmitted to the infant congenitally, intrapartum, or postpartum through close contact with the mother or via breast milk. The extent to which these should be evaluated for when a woman presents late in gestation or at time of delivery varies on a case-by-case basis.
Hepatitis C virus (HCV)
The estimated prevalence of HCV infection in Canada is between 0.5% and 1.0%[35]. Injection drug use is the predominant risk factor and present in at least two-thirds of cases[36]. Other risk factors include any substance use, being born to a mother with HCV infection, having been born in a country with high HCV seroprevalence, or engaging in sexual behaviour where blood may be present. The average risk for perinatal HCV transmission is approximately 6%[37]. Factors that can increase this risk include HIV co-infection, higher maternal HCV viral load, use of fetal scalp monitoring, prolonged rupture of membranes, being the second-born twin, and infant female sex. There is currently no evidence that mode of delivery impacts transmission risk, no evidence that HCV can be transmitted via breast milk, and no evidence for the use of direct-acting antiviral medications to prevent vertical HCV transmission. In the United States, the Society for Maternal-Fetal Medicine recommends routine screening for HCV in pregnancy, and this strategy may be adopted in Canada in the near future[38]. In the interim, a risk-based approach to screening is recommended[36][39].
Herpes simplex virus (HSV)
HSV is an important consideration due to the severity of neonatal disease, the efficacy of prophylactic antiviral therapy during pregnancy in women with recurrent genital HSV, the efficacy of Caesarean section in reducing vertical transmission when women have suggestive prodromal symptoms or active lesions at delivery, and the availability of antiviral treatment for affected neonates[13][40]. When a mother is noted to have lesions potentially due to HSV at or near time of delivery, polymerase chain reaction (PCR) testing of lesion samples should be conducted[40].
Cytomegalovirus (CMV)
CMV is the most common congenital infection, affecting approximately 0.5% of newborns in Canada. Women experiencing adverse social determinants of health, including those with limited or no antenatal care, may be at higher risk of acquiring CMV infection in pregnancy. While there is presently no Canada-wide recommendation for routine CMV screening in newborns, infants who have symptoms compatible with congenital CMV, such as unexplained intrauterine growth restriction, hepatitis, petechial rash with thrombocytopenia, or microcephaly, and those who fail their newborn hearing screen, should have urine or saliva CMV PCR testing before they are 3 weeks old to assess for congenital CMV infection[41].
Recommendations
Testing mothers for infectious disease at or immediately following childbirth—or infants immediately post-birth if their mothers are not available—is recommended in the following circumstances:
- When routine prenatal tests for infection have not been performed or results are not available.
- When early prenatal tests were negative but the mother, or her sexual partner(s), is deemed to have been at ongoing or subsequent risk for acquiring infection. Indicators for ongoing maternal risk include: use of intoxicating substances (particularly injection drugs) during pregnancy; sharing drug paraphernalia (injection or non-injection-related); having new, multiple, or anonymous sexual partners; having a documented sexually transmitted infection (STI); or having a history of being homeless or incarcerated.
- When local epidemiology indicates that repeat testing for a particular pathogen late in gestation is advisable for all women.
Baseline evaluation for infections in mothers who are available for testing late in gestation or at time of childbirth includes:
- Testing for human immunodeficiency virus (HIV), hepatitis B virus (HBV), hepatitis C virus (HCV), syphilis, Chlamydia trachomatis, and Neisseria gonorrhoeae (Table 1).
- Performing:
- Recto-vaginal swab for Streptococcus agalactiae (GBS) culture as soon as possible after 36+0 weeks gestation to allow for intrapartum prophylaxis-related decisions;
- Polymerase chain reaction (PCR) testing of maternal genital lesions suggestive of herpes simplex virus (HSV), if present at or near the time of labour.
Baseline testing in infants pending maternal test results for HIV, HBV, HCV, and syphilis is generally not required. When a mother tests positive for any of these pathogens, or if her history suggests risk for late gestational infection, follow-up testing for both the mother and infant is recommended, in consultation with an infectious diseases (ID) expert.
Table 1. Routine blood-borne and sexually transmitted infection workup of mothers with inadequate prenatal care presenting late in gestation or at time of labour
|
Pathogen |
Test |
Testing methodology |
|---|---|---|
|
HIV |
Serology* |
STAT†; POCT with confirmatory serology preferred (if not available, standard serology)‡ |
|
|
PCR or viral load |
Selectively for women deemed at high risk of late gestation HIV infection, where empiric infant antiretroviral prophylaxis or pre-emptive therapy is being considered§ |
|
HBV |
HBsAg* |
STAT¶ |
|
HCV |
Serology |
STAT testing not required |
|
Syphilis |
Serology* |
STAT**; POCT with confirmatory serology preferred (if not available, standard serology)‡ |
|
C. trachomatis |
NAAT |
Self-collected vaginal swab†† OR |
|
|
NAAT |
Health care provider cervical swab OR |
|
|
NAAT |
First void urine |
|
N. gonorrhoeae |
NAAT or culture* |
Self-collected vaginal swab†† OR |
|
|
NAAT or culture* |
Health care provider endo cervical swab OR |
|
|
NAAT* |
First void urine |
HBV Hepatitis B virus; HBsAg Hepatitis B surface antigen; HCV Hepatitis C virus; HIV Human immunodeficiency virus; NAAT Nucleic acid amplification test; PCR Polymerase chain reaction; POCT Point-of-care test
* STAT testing recommended because results impact immediate maternal and infant management. HBsAg and HIV serology should be available within 6 to 12 h of birth, and syphilis serology results before discharging infant.
† If STAT testing is not available, consult a paediatric HIV expert regarding management pending test results.
‡ POCT testing can be done at the bedside with near-instant result availability.
-
Warranted for situations where the mother is deemed to be at high risk for recent infection (before seroconversion; see text for risk factors).
¶ See Figure 2 for management according to availability of STAT test results.
** If STAT testing is not available, assurance of close follow-up of the newborn is essential such that appropriate management can be implemented when results become available.
†† Self-collected vaginal swab preferred; health care provider cervical swab a reasonable alternative; first void urine is an option but logistically more challenging.
Baseline evaluation for infections in infants whose mothers are not available for testing includes:
- Testing for HIV, HBV, HCV, and syphilis (Table 2).
For neonates who develop conjunctivitis soon after birth, obtain conjunctival swabs for a C. trachomatis nucleic acid amplification test (NAAT) or culture, and for gonococcal culture. Perform appropriate bacterial cultures also.
For infants who develop pneumonia during the first 6 to 8 weeks of life, obtain a nasopharyngeal swab for C. trachomatis NAAT.
Consult with a local ID epidemiologist or microbiologist to ensure that appropriate samples are collected. Routine testing for C. trachomatis or N. gonorrhoeae is not required when clinical symptoms are absent.
Table 2. Routine blood-borne and sexually transmitted infection workup of infants whose mothers are not available for testing
|
Pathogen |
Test |
Test rationale and methodology |
|
|---|---|---|---|
|
HIV |
Serology*† |
Assesses for evidence of maternal infection‡ POCT preferred with confirmatory serology (if not available, standard serology)§ |
|
|
|
PCR or viral load |
Selectively, when serologic screening is reactive or when maternal history is concerning for possible late gestational acquisition of HIV infection (pre-seroconversion)¶ |
|
|
HBV |
Anti-HBs, (HbsAg) | Primarily to indirectly establish maternal immunity status ‡ | |
|
HCV |
Serology ** |
Assesses for evidence of maternal infection or immunity‡ |
|
|
Syphilis |
Serology*†† |
Assesses for evidence of maternal‡ and infant infection POCT with confirmatory serology preferred (if not available, standard serology)§ |
Anti-HBs Anti-hepatitis B surface antibody; HBV Hepatitis B virus; HBsAg Hepatitis B surface antigen; HCV Hepatitis C virus; HIV Human immunodeficiency virus; PCR Polymerase chain reaction; POCT Point-of-care test
* STAT testing recommended because results impact immediate infant management. HBsAg and HIV serology should be available within 6 to 12 h of birth, and syphilis serology results before discharging the infant.
† If STAT testing is not available, consult a paediatric HIV expert regarding management pending test results.
‡ Anti-HBs is reflective of transplacental maternal antibody; note that a reactive HbsAg in the newborn is not diagnostic of infection as this may reflect transient non-intact viral particles from the mother.
§ POCT testing can be done at the bedside with near-instant result availability.
¶ A negative result does not exclude perinatally acquired HIV infection.
** STAT testing is not required because immediate management is not impacted. All infants who test positive serologically should have follow-up testing as outlined in reference 17.
†† If STAT testing is not available, assurance of close follow-up of the newborn is essential such that appropriate management can be implemented when results become available.
Managing infants at risk for infection, with follow-up testing, is recommended in the following circumstances:
- HIV: When baseline maternal (or infant) HIV serology is reactive, or maternal molecular testing is positive, the infant should receive an HIV PCR or viral load test and prophylactic or pre-emptive treatment with cART initiated within 6 to 12 h of birth. This recommendation is based on the high risk for perinatal HIV transmission (Figure 1). When maternal testing is negative or not available and there is concern for risk based on recent history, consider initiating antiretroviral therapy for the infant before test results are received. Consultation and follow-up involving a paediatric HIV or ID expert is recommended in all such cases. (For information on Canadian paediatric HIV experts and clinics, consult the Canadian Pediatric and Perinatal HIV/AIDS Research Group website: https://www.cparg.ca/). Exclusive formula feeding is recommended until HIV infection has been excluded in the mother.
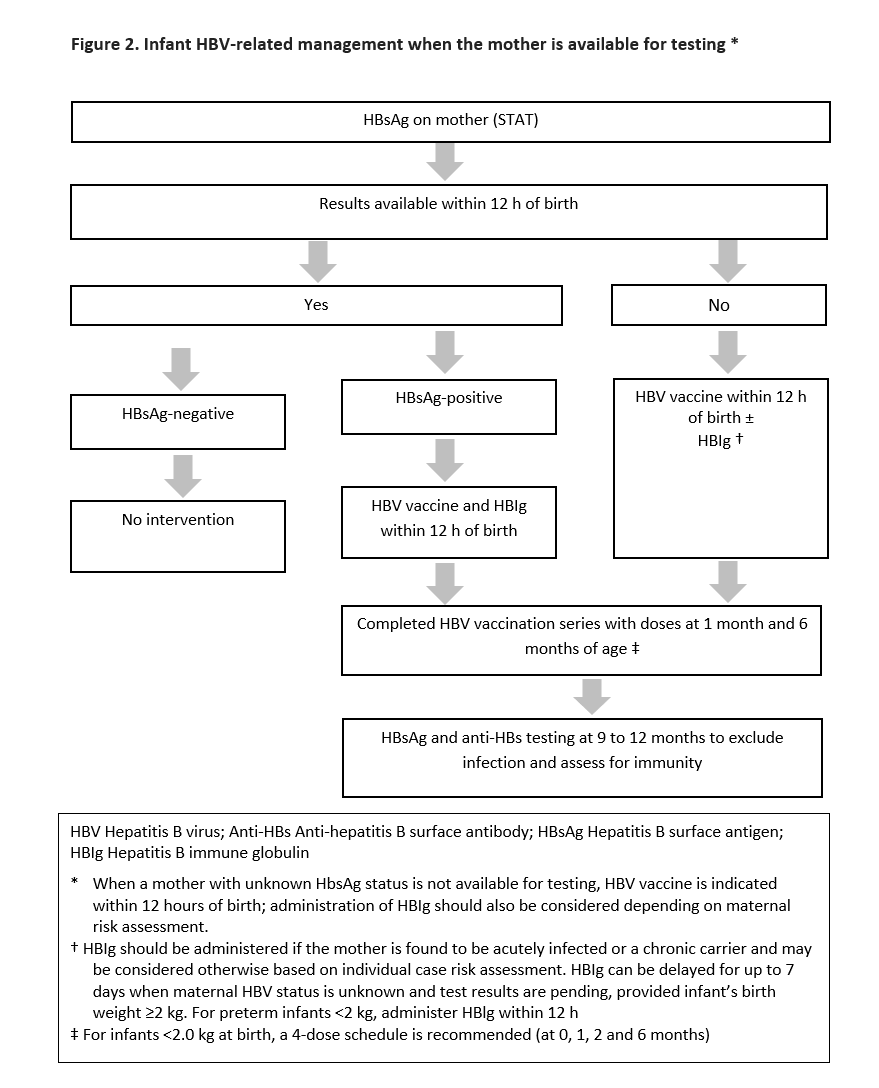
- HBV: Testing and treatment recommendations derived from the Canadian Immunization Guide are shown in Figure 2 ( https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-4-active-vaccines/page-7-hepatitis-b-vaccine.html ). Breastfeeding is not contraindicated.
- HCV: No treatment is recommended and breastfeeding is not contraindicated. Breastfeeding should be temporarily interrupted if the mother has cracked or bleeding nipples. Follow-up with appropriate testing is recommended, as delineated in the CPS statement “The management of infants, children, and youth at risk for hepatitis C virus (HCV) infection”.
- HSV: Management of exposed infants is outlined in the CPS statement “Prevention and management of neonatal herpes simplex virus infections ”.
- C. trachomatis: Empiric treatment of exposed asymptomatic infants is not warranted. Close follow-up for clinical symptoms of disease is appropriate. Infants who develop conjunctivitis or pneumonia should have clinical samples obtained for culture or molecular detection, depending on local recommendations. Those who test positive should be treated with erythromycin base or ethylsuccinate (50 mg/kg/day in 4 divided doses) for 14 days or azithromycin (20 mg/kg once daily) for 3 days.
- N. gonorrhoeae: A single dose of intramuscular (IM) or intravenous (IV) ceftriaxone (50 mg/kg, to a maximum 125 mg) should be administered to asymptomatic newborns whose mothers test positive but did not receive treatment before delivery. A single dose of IV or IM cefotaxime (100 mg/kg) is an acceptable alternative when ceftriaxone is contraindicated. For infants born to mothers with an unknown history who are not available for testing, empiric treatment cannot be recommended, but they should be followed closely and managed based on symptoms.
- S. agalactiae: Manage term infants in accordance with the CPS statement “Management of term infants at increased risk for early onset bacterial sepsis”.
- Treponema pallidum: If the mother has reactive syphilis serology, or she is not available for testing, or she did not receive appropriate treatment before or during pregnancy and her infant’s serology is reactive, the infant should be investigated and treated. A CPS statement on syphilis is expected in 2023.
Figure 1. HIV-related testing and management
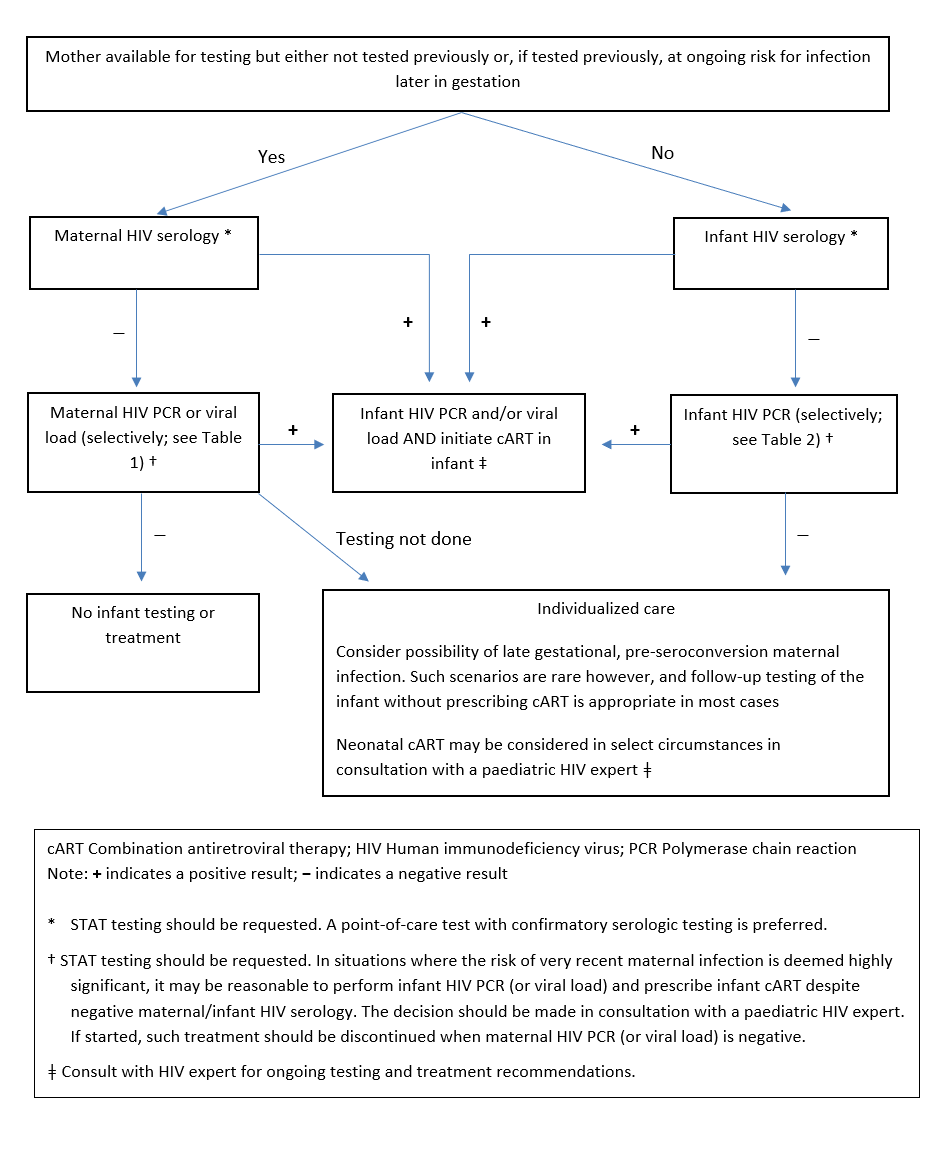
Figure 2. Infant HBV-related management when the mother is available for testing *
Acknowledgements
This position statement has been reviewed by the Community Paediatrics, Fetus and Newborn, and First Nations, Inuit and Métis Health Committees of the Canadian Paediatric Society. It was also reviewed by the College of Family Physicians of Canada (CFPC), and by members of the Society of Obstetricians and Gynaecologists of Canada’s (SOGC’s) Clinical Practice Obstetrics and Infectious Disease Committees. It has been reviewed and endorsed by the Canadian Pediatric and Perinatal HIV/AIDS Research Group (CPARG).
CANADIAN PAEDIATRIC SOCIETY INFECTIOUS DISEASES AND IMMUNIZATION COMMITTEE (2021-2022)
Members: Michelle Barton MD; Ari Bitnun MD; Sergio Fanella MD; Laura Sauvé MD (Chair); Raphael Sharon MD (Board Representative); Karina A. Top MD
Liaisons: Ari Bitnun MD, Canadian Paediatric and Perinatal HIV/AIDS Research Group; Cheryl Foo MD, Immunization Monitoring Program, ACTive (IMPACT); Fahamia Koudra MD, College of Family Physicians of Canada; Yvonne Maldonado MD, Committee on Infectious Diseases, American Academy of Pediatrics; Dorothy L. Moore MD, National Advisory Committee on Immunization (NACI); Marina Salvadori MD, Public Health Agency of Canada; Isabelle Viel-Thériault MD, Committee to Advise on Tropical Medicine and Travel (CATMAT)
Consultant: Noni E. MacDonald MD
Principal authors: Ari Bitnun MD, Laura Sauvé MD, Sergio Fanella MD
References
- Levitt A, Mermin J, Jones CM, See I, Butler JC. Infectious diseases and injection drug use: Public health burden and response. J Infect Dis 2020;222(Suppl 5):S213-7. DOI: 10.1093/infdis/jiaa432.
- Heaman MI, Green CG, Newburn-Cook CV, Elliott LJ, Helewa ME. Social inequalities in use of prenatal care in Manitoba. J Obstet Gynaecol Can 2007;29(10):806-16. DOI: 10.1016/s1701-2163(16)32637-8.
- Carter Ramirez A, Liauw J, Cavanagh A, et al. Quality of antenatal care for women who experience imprisonment in Ontario, Canada. JAMA Netw Open 2020;3(8):e2012576. DOI: 10.1001/jamanetworkopen.2020.12576.
- Jarvis C, Munoz M, Graves L, Stephenson R, D’Souza V, Jimenez V. Retrospective review of prenatal care and perinatal outcomes in a group of uninsured pregnant women. J Obstet Gynaecol Can 2011;33(3):235-43. DOI: 10.1016/s1701-2163(16)34824-1.
- Wilson-Mitchell K, Rummens JA. Perinatal outcomes of uninsured immigrant, refugee and migrant mothers and newborns living in Toronto, Canada. Int J Environ Res Public Health 2013;10(6):2198-213. DOI: 10.3390/ijerph10062198.
- Khanlou N, Haque N, Skinner A, Mantini A, Kurtz Landy C. Scoping review on maternal health among immigrant and refugee women in Canada: Prenatal, intrapartum, and postnatal care. J Pregnancy 2017;2017:8783294. DOI: 10.1155/2017/8783294.
- Little M, Shah R, Vermeulen MJ, Gorman A, Dzendoletas D, Ray JG. Adverse perinatal outcomes associated with homelessness and substance use in pregnancy. CMAJ 2005;173(6):615-8. DOI: 10.1503/cmaj.050406.
- Knight E, Morris M, Heaman M. A descriptive study of women presenting to an obstetric triage unit with no prenatal care. J Obstet Gynaecol Can 2014;36(3):216-22. DOI: 10.1016/S1701-2163(15)30629-0.
- Heaman MI, Martens PJ, Brownell MD, et al. Inequities in utilization of prenatal care: A population-based study in the Canadian province of Manitoba. BMC Pregnancy Childbirth 2018;18(1):430. DOI: 10.1186/s12884-018-2061-1.
- Heaman MI, Moffatt M, Elliott L, et al. Barriers, motivators and facilitators related to prenatal care utilization among inner-city women in Winnipeg, Canada: A case-control study. BMC Pregnancy Childbirth 2014;14:227. DOI: 10.1186/1471-2393-14-227.
- Nussey L, Hunter A, Krueger S, et al. Sociodemographic characteristics and clinical outcomes of people receiving inadequate prenatal care: A retrospective cohort study. J Obstet Gynaecol Can 2020;42(5):591-600. DOI: 10.1016/j.jogc.2019.08.005.
- Malebranche M, Norrie E, Hao S, et al. Antenatal care utilization and obstetric and newborn outcomes among pregnant refugees attending a specialized refugee clinic. J Immigr Minor Health 2020;22(3):467-75. DOI: 10.1007/s10903-019-00961-y.
- Allen UD, Robinson JL, Bitnun A, McDonald J; Canadian Paediatric Society, Infectious Diseases and Immunization Committee. Prevention and management of neonatal herpes simplex virus infections. Updated March 6, 2020: https://www.cps.ca/en/documents/position/prevention-management-neonatal-herpes-simplex-virus-infections.
- Moore DL, MacDonald NE; Canadian Paediatric Society, Infectious Diseases and Immunization Committee. Preventing ophthalmia neonatorum. Paediatr Child Health 2015;20(2):93-96: https://cps.ca/en/documents/position/ophthalmia-neonatorum.
- Fanella S, Bitnun A, Barton-Forbes M, Sauvé L; Canadian Paediatric Society, Infectious Diseases and Immunization Committee. Congenital syphilis – Avoiding missed opportunities (in press).
- Jefferies AL; Canadian Paediatric Society, Fetus and Newborn Committee. Management of term infants at increased risk for early onset bacterial sepsis. Paediatr Child Health 2017;22(4):223-28: https://cps.ca/en/documents/position/management-infant-sepsis.
- Bitnun A; Canadian Paediatric Society, Infectious Diseases and Immunization Committee. The management of infants, children, and youth at risk for hepatitis C virus (HCV) infection. Paediatr Child Health 2021(7):440 (Abstract): https://cps.ca/en/documents/position/the-management-of-hepatitis-c-virus.
- Public Health Agency of Canada. Sexually Transmitted and Blood-borne Infections: Guides for Health Professionals. Last update August 31, 2017: https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/canadian-guidelines.htm (Accessed September 29, 2022).
- Public Health Agency of Canada. Primary Care Management of Hepatitis B – Quick Reference (HBV-QR): https://www.canada.ca/en/public-health/services/reports-publications/primary-care-management-hepatitis-b-quick-reference.html (Accessed September 29, 2022).
- American Academy of Pediatrics, Committee on Infectious Diseases. Hepatitis B. In: Kimberlin DW, Barnett ED, Lynfield R, Sawyer MH, eds. Red Book: 2021-2024. Itasca, IL: American Academy of Pediatrics; 2021.
- Bitnun A, Lee T, Brophy J, et al. Missed opportunities for prevention of vertical HIV transmission in Canada, 1997-2016: A surveillance study. CMAJ Open 2018;6(2):E202-10. DOI: 10.9778/cmajo.20180016.
- Forbes JC, Alimenti AM, Singer J, et al. A national review of vertical HIV transmission. AIDS 2012;26(6):757-63. DOI: 10.1097/QAD.0b013e328350995c.
- Nielsen-Saines K, Watts DH, Veloso VG, et al. Three postpartum antiretroviral regimens to prevent intrapartum HIV infection. N Engl J Med 2012;366(25):2368-79. DOI: 10.1056/NEJMoa1108275.
- Public Health Agency of Canada. Syphilis in Canada: Technical Report on Epidemiological Trends, Determinants and Interventions. May 2020: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/syphilis-epidemiological-report/syphilis-eng.pdf (Accessed August 23, 2022).
- Aho J, Lybeck C, Tetteh A, et al. Rising Syphilis Rates in Canada, 2011-2020. Can Comm Dis Rep 2022;48(2/3):52-60. DOI: 10.14745/ccdr.v48i23a01.
- Public Health Agency of Canada. Infectious Syphilis and Congenital Syphilis in Canada, 2020 (infographic): https://www.canada.ca/en/public-health/services/publications/diseases-conditions/infectious-syphilis-congenital-syphilis-canada-2020.html (Accessed August 23, 2022).
- American Academy of Pediatrics, Committee on Infectious Diseases. Syphilis. In: Kimberlin DW, Barnett ED, Lynfield R, Sawyer MH, eds. Red Book: 2021. Itasca, IL: American Academy of Pediatrics; 2021..
- Kimball A, Torrone E, Miele K, et al. Missed Opportunities for Prevention of Congenital Syphilis—United States, 2018. MMWR Morb Mortal Wkly Rep 2020;69(22):661-65. DOI: 10.15585/mmwr.mm6922a1.
- Public Health Agency of Canada. Chlamydia, Gonorrhea and Infectious Syphilis in Canada, 2018: Infographic: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/sexually-transmitted-infections-canada-2018-infographic.html (Accessed August 23, 2022).
- Public Health Agency of Canada. Report on Sexually Transmitted Infections in Canada, 2017. October 2019: https://www.canada.ca/content/dam/hc-sc/documents/services/publications/diseases-and-conditions/sexually-transmitted-infections-canada-2017-infographic/STI_2017_20191113_EN.PDF (Accessed August 23, 2022).
- Hammerschlag MR, Chandler JW, Alexander ER, English M, Koutsky L. Longitudinal studies on chlamydial infections in the first year of life. Pediatr Infect Dis 1982;1(6):395-401. DOI: 10.1097/00006454-198211000-00007.
- Schachter J, Grossman M, Sweet RL, Holt J, Jordan C, Bishop E. Prospective study of perinatal transmission of Chlamydia trachomatis. JAMA 1986;255(24):3374-7.
- Galega FP, Heymann DL, Nasah BT. Gonococcal ophthalmia neonatorum: The case for prophylaxis in tropical Africa. Bull World Health Organ 1984;62(1):95-98.
- Laga M, Plummer FA, Nzanze H, et al. Epidemiology of ophthalmia neonatorum in Kenya. Lancet 1986;2(8516):1145-49. DOI: 10.1016/s0140-6736(86)90544-1.
- Trubnikov M, Yan P, Archibald C. Estimated prevalence of hepatitis C virus infection in Canada, 2011. Can Commun Dis Rep2014;40(19):429-36. DOI: 10.14745/ccdr.v40i19a02.
- Canadian Network on Hepatitis C; Blueprint Writing Committee and Working Groups. Blueprint to Inform Hepatitis C Elimination Efforts in Canada. May 2019: https://www.canhepc.ca/sites/default/files/media/documents/blueprint_hcv_2019_05.pdf (Accessed August 23, 2022).
- Benova L, Mohamoud YA, Calvert C, Abu-Raddad LJ. Vertical transmission of hepatitis C virus: Systematic review and meta-analysis. Clin Infect Diseases 2014;59(6):765-73. DOI: 10.1093/cid/ciu447.
- Society for Maternal-Fetal Medicine; Dotters-Katz SK, Kuller JA, Hughes BL. Society for Maternal-Fetal Medicine Consult Series #56: Hepatitis C in pregnancy—Updated guidelines: Replaces consult number 43, November 2017. Am J Obste Gynecol 2021;225(3):B8-18. DOI: 10.1016/j.ajog.2021.06.008.
- Ha S, Totten S, Pogany L, Wu J, Gale-Rowe M. Hepatitis C in Canada and the importance of risk-based screening. Can Commun Dis Rep 2016;42(3):57-62. DOI: 10.14745/ccdr.v42i03a02.
- Money DM, Steben M. No. 208—Guidelines for the Management of herpes simplex virus in pregnancy. J Obstet Gynaecol Can 2017;39(8):e199-e205. DOI: 10.1016/j.jogc.2017.04.016.
- Barton M, Forrester AM, McDonald J; Canadian Paediatric Society, Infectious Diseases and Immunization Committee. Update on congenital cytomegalovirus infection: Prenatal prevention, newborn diagnosis, and management. Paediatr Child Health 2020;25(6):395 (Abstract): https://cps.ca/en/documents/position/update-on-congenital-cytomegalovirus-infection-prenatal-prevention-newborn-diagnosis-and-management.
Disclaimer: The recommendations in this position statement do not indicate an exclusive course of treatment or procedure to be followed. Variations, taking into account individual circumstances, may be appropriate. Internet addresses are current at time of publication.