Practice point
Management of brief resolved unexplained events (BRUE) in infants: A practice point for evidence-based practice and family-centred care

Posted: Jul 6, 2026
Principal author(s)
Nassr Nama MD MSc, Kara Picco MD, Olivia Ostrow MD, Joel S. Tieder MD MPH, Peter J. Gill MD DPhil MSc; Canadian Paediatric Society, Hospital Paediatrics Section Executive
Abstract
In 2016, the American Academy of Pediatrics (AAP) defined “brief resolved unexplained events” (BRUE) as brief, sudden, spontaneously resolving episodes in infants younger than 1 year of age, characterized by a change in colour, breathing, muscle tone, or responsiveness, and unexplained after focused clinical evaluation. BRUE replaced a broader, less specific term: “apparent life-threatening events” (ALTE). An AAP guideline offered risk-based recommendations grounded in older ALTE literature. A more precise BRUE definition has since improved understanding of outcomes and management. BRUE-related publications from 2016 to 2025 were systematically reviewed for this practice point, and evidence from twenty-four eligible studies has been summarized to produce the ‘best practice’ points offered here. Serious diagnoses are rare, mortality is comparable to that in the general population, and most well-appearing infants can be safely managed without hospital admission. This practice point emphasizes the importance of a careful history and physical exam to exclude alternative diagnoses and recommends against routine testing unless clinically indicated because overtesting can lead to false positives and unnecessary interventions.
Keywords: Brief resolved unexplained events (BRUE); Infants; Resource stewardship
Diagnostic criteria
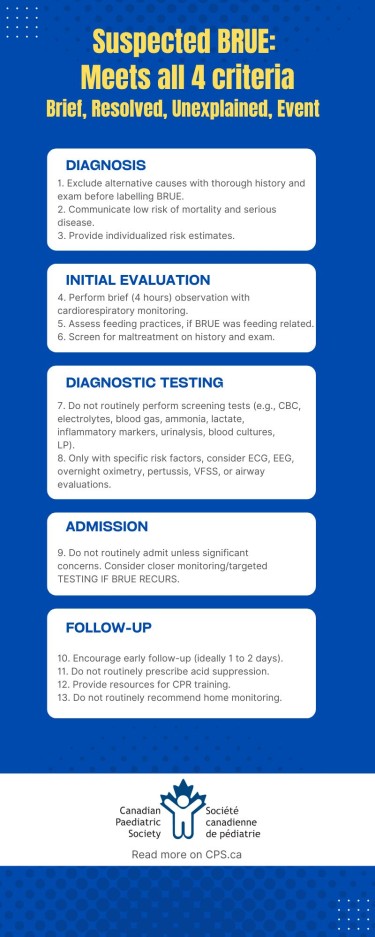
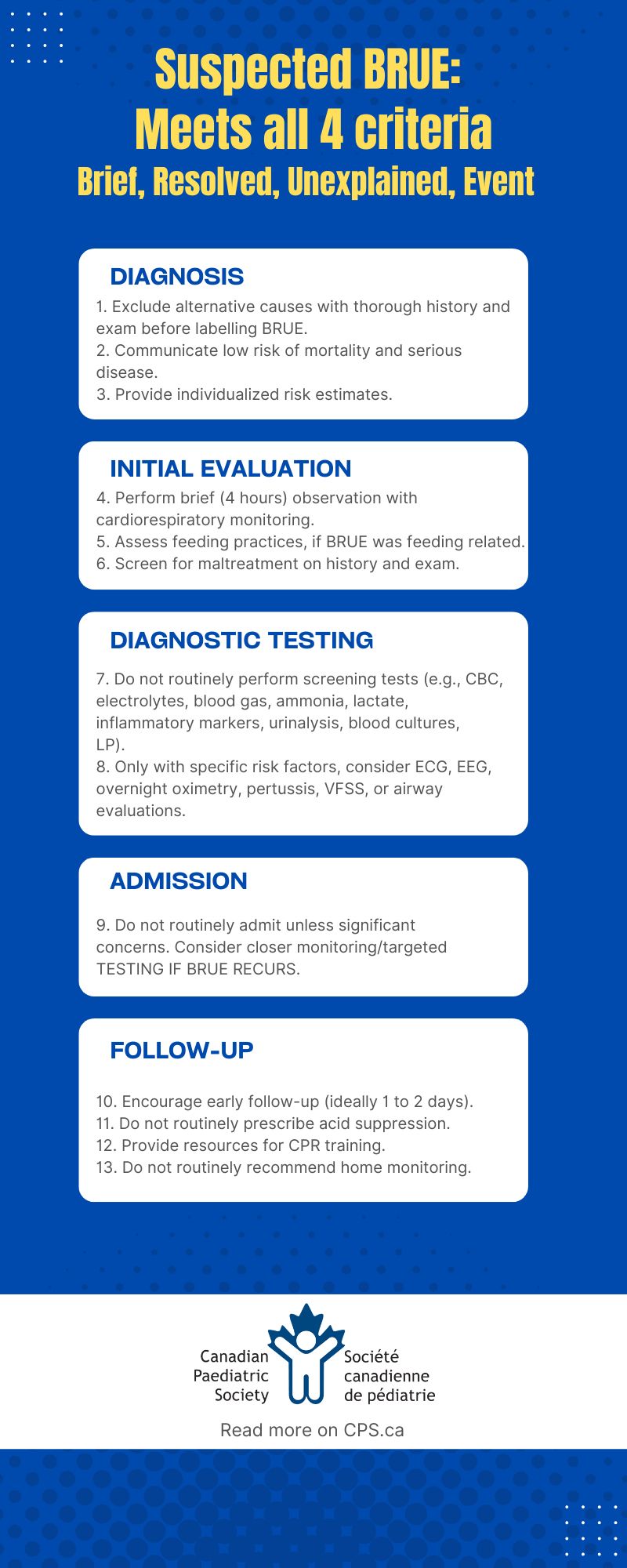
Best practice point 1: Rule out an episode’s alternative causes based on a thorough history and physical exam before labelling as BRUE.
BRUE is a diagnosis of exclusion in infants <1 year of age and based on criteria shown in Table 1 and Figure 1[1]. A focused history and physical exam remain the most effective tools for ruling out other potential diagnoses (Figure 2). Clinicians should obtain detailed witness accounts and investigate triggers, feeding practices, growth, development, and risk factors, particularly for neurological disorders, apnea, and maltreatment[2][3].
Table 1. Diagnostic criteria for brief resolved unexplained event (BRUE) in infants <1 year
|
Component |
Definition |
Exclusions |
|
Brief |
Event lasts <1 minute |
Prolonged or recurrent events, or an episode requiring professional medical resuscitation |
|
Resolved |
Infant returns to baseline with normal vital signs and physical exam at the time of medical assessment |
Persistent abnormal findings on examination (e.g., lethargy, respiratory distress, abnormal tone) |
|
Unexplained |
No identifiable cause after a thorough history and exam |
Identifiable cause, like an infection, reflux, seizure, or airway anomaly |
|
Event |
Includes ≥1 of these signs:
|
Benign conditions like periodic breathing, isolated perioral cyanosis, breath-holding spells, or postictal states |
Information drawn from reference 1
Figure 1. Structured evaluation for suspected brief resolved unexplained event (BRUE), and risk factors for alternate or underlying diagnoses
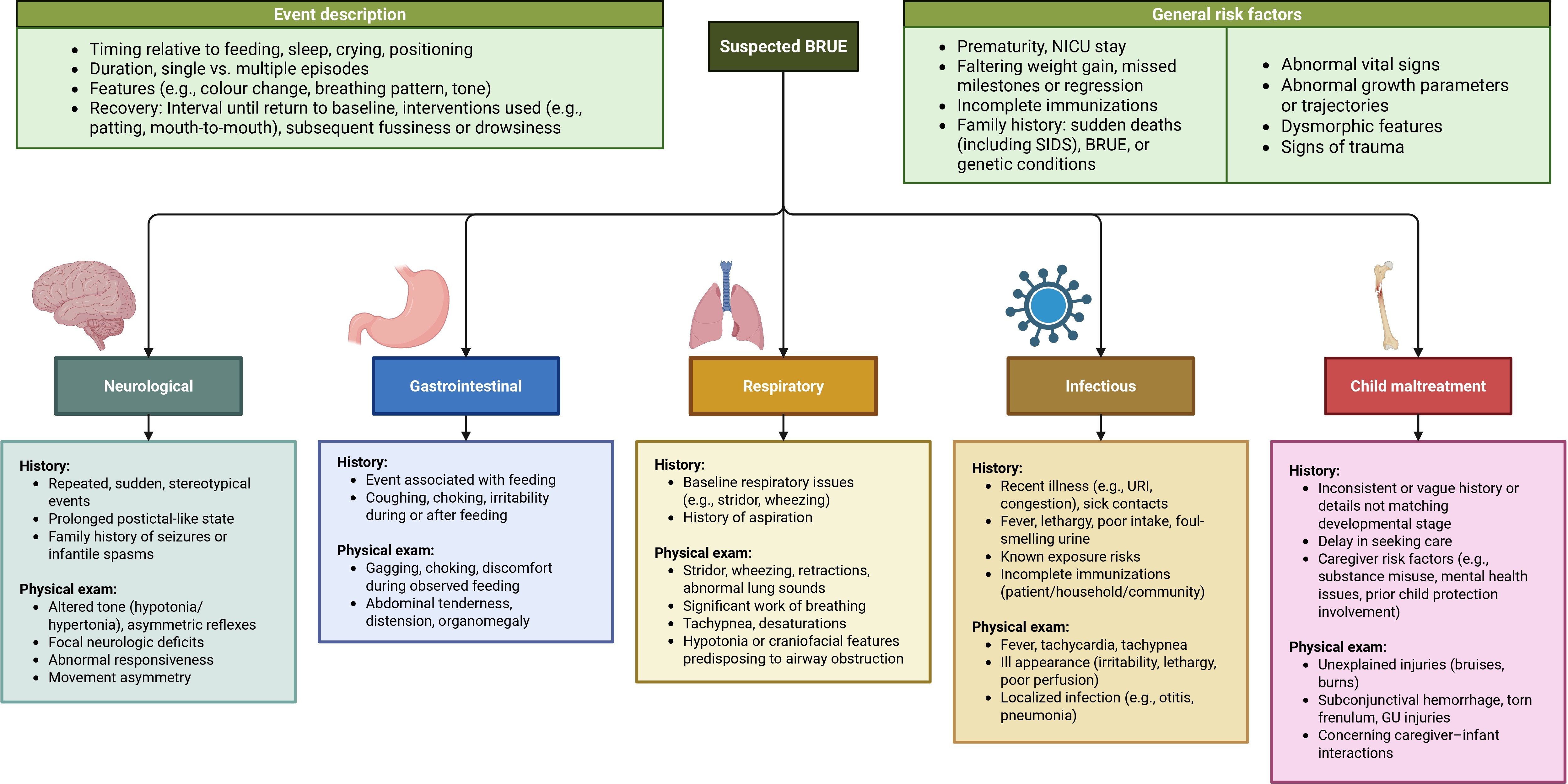 Information drawn from references 1,2
Information drawn from references 1,2
BRUE, brief resolved unexplained event; GU, genitourinary; NICU, neonatal intensive care unit; SIDS, sudden infant death syndrome; URI, upper respiratory infection
Figure 2. Differential diagnoses in patients presenting with suspected brief resolved unexplained event (BRUE)
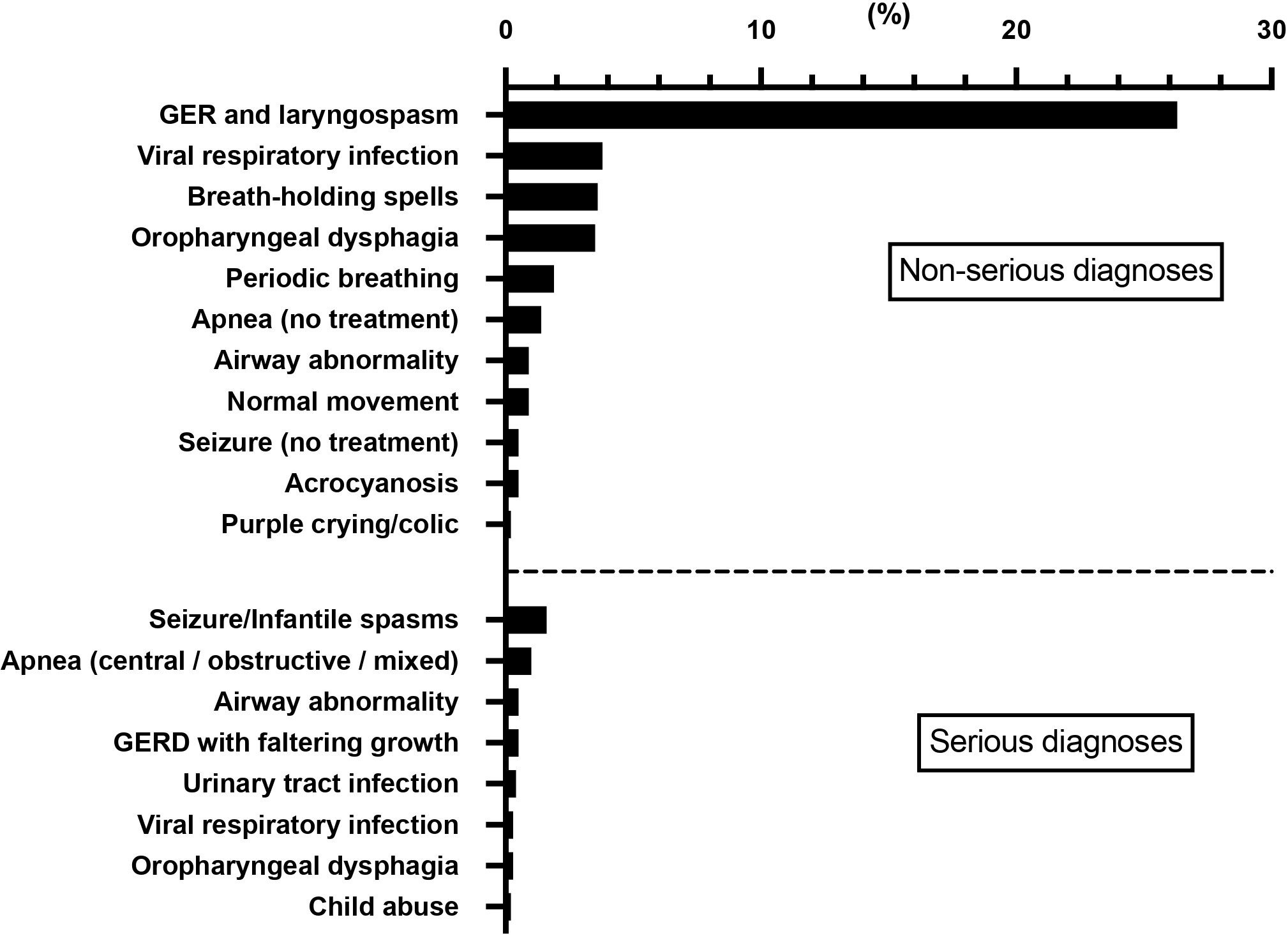
Data are pooled for serious diagnoses (12 studies, N=4958) and non-serious diagnoses (two studies, N=3,078)[3][4].
CBC, complete blood count; CPR, cardiopulmonary resuscitation; ECG, electrocardiogram; EEG, electroencephalogram; LP, lumbar puncture; VFSS, videofluoroscopic swallow study
Clinical outcomes and risk stratification
Best practice point 2: Communicate to caregivers the low risk for mortality and serious underlying disease. Consider longer observation or closer outpatient follow-up for recurrent BRUEs, which indicate greater risk for serious conditions.
BRUE is not associated with sudden unexpected infant death, but rather with mortality mirroring the general population (1 in 1851 over 3 months)[4]. Serious underlying diagnoses are, most commonly, epilepsy or apnea (but are still rare at about 6%), while invasive bacterial infections, cardiac, and metabolic disorders are exceedingly uncommon (Figure 2)[5][6]. More frequently, mild feeding difficulties or reflux are identified[6][7]. Recurrent BRUEs (14%) are associated with a higher risk for serious pathology[6][8]-[10].
Best practice point 3: Use recently developed tools to stratify risk and provide precise, individualized risk estimates for serious conditions and recurrence.
Risk stratification in AAP guidance is limited because it classifies over 90% of infants as higher risk while yielding a low positive predictive value[9][11][12]. Published studies have not shown clinically meaningful differences in outcomes between AAP’s “lower” and “higher” risk infants, and age alone does not independently predict risk after initial evaluation. Tools developed recently and validated in Canadian and U.S. populations provide more precise risk estimates[9][12][13]. By accommodating varying risk tolerances rather than a binary classification of higher and lower risk, these tools can facilitate shared decision-making that includes caregiver priorities and social context (e.g., access to follow-up, available support).
Approach to clinical evaluation
(Figure 3)
Initial assessment
Best practice point 4: Perform brief (4 hours) observation with cardiorespiratory monitoring.
After history and exam exclude underlying causes, brief monitoring helps identify recurrent events or evolving symptoms, and can reassure caregivers[1][2][14]. Prolonged monitoring risks false alarms, alarm fatigue, and increased caregiver anxiety. Because this period of observation may be challenging in a primary care setting, an emergency department (ED) is often the most appropriate setting for initial evaluation.
Best practice point 5: Assess feeding practices, particularly if BRUE was temporally feeding-related, but do not admit solely for feeding evaluation.
For events related to feeding, obtain a detailed history and directly observe feeding. This identifies modifiable factors (e.g., overfeeding, poor latch, positioning), guide adjustments, and help determine the need for further testing (e.g., videofluoroscopic swallow study [VFSS])[15][16].
Best practice point 6: Screen for maltreatment with detailed history and physical exam.
Clinicians must remain alert to signs of abuse or psychosocial ‘red flags’, which should trigger evaluation by social work or child protection and appropriate diagnostic testing[17]-[19].
Diagnostic testing
Best practice point 7: Avoid routine non-specific screening tests.
Routine testing (complete blood count, electrolytes, blood gas, ammonia, lactate, inflammatory markers, urinalysis, blood and urine cultures, lumbar puncture) is extremely low yield (only 1% to 5%) for identifying BRUE etiologies, and can cause false positives and unnecessary investigations and admissions[20]-[24]. Clinicians should discuss potential harms and limited benefits with families who are seeking reassurance through testing[16][25]-[28].
Best practice point 8: Perform targeted testing only when specific historical or clinical factors indicate a particular condition, including:
- Electrocardiogram (ECG) for abnormal exam or concerning family history (arrhythmias, sudden unexplained death). Despite prior AAP suggestions, routine ECG without risk factors rarely provides clinically meaningful information[10][16][20][22][24].
- Electroencephalogram (EEG) for suspected seizures, abnormal exam, or concerning family history[20][22][24][29].
- Overnight oximetry for baseline respiratory issues or risk factors for apnea[24][30].
- Pertussis testing only during local outbreaks or for infants in under-immunized communities[8][10][22][31]-[34].
- Speech-language pathology (SLP) referral and VFSS when initial feeding assessments indicate aspiration risk. Although VFSS identifies silent laryngeal penetration in some infants with BRUE, the clinical significance of these findings remains unclear[20][22][24][28][35].
- Airway evaluation for recurrent respiratory symptoms or suspected airway abnormalities[16][24].
Respiratory virus panels occasionally provide an explanation, but rarely change management[8][10][22][24][31][33]. Because recurrent BRUE is a risk factor for serious diagnoses (particularly seizures and apnea), clinicians may consider EEG and overnight oximetry testing for these infants.
Hospital admission
Best practice point 9: Do not routinely admit infants unless there are concerns about maltreatment, inadequate follow-up, or significant comorbidities.
Hospitalizing well-appearing infants without specific risk factors does not reliably identify serious causes, which often require more time to manifest[5]. Observing recurrences during hospitalization rarely provides diagnostic clarity[5]-[7]. Over the past decade, hospital admission rates for BRUE have decreased without an increase in return ED visits, suggesting this approach does not compromise infant safety[36]-[38].
Admission may be suggested for families struggling with diagnostic uncertainty and should be balanced with hospitalization risks[25][26][28][39]. If admitting, clearly communicate expectations to families, emphasizing that hospitalization typically does not identify an underlying diagnosis.
Follow-up
Best practice point 10: Arrange for prompt outpatient follow-up (e.g., within few days) to reassess clinical status and address evolving symptoms[1].
Regular contact with a primary care provider can mitigate anxiety, clarify diagnostic uncertainties, and reduce unnecessary readmissions[20]. Infants with recurrent episodes or other red flags may require further testing or specialty referrals, and decisions about outpatient versus inpatient evaluations often hinge on resource availability. When timely primary care follow-up is not feasible, reassessment may reasonably occur via a walk-in clinic or virtual/telephone visit, depending on local access and resources.
Best practice point 11: Avoid acid suppression for BRUE. Even when gastroesophageal reflux (GER) is suspected clinically, treatment does not reduce BRUE recurrence and carries risks.
Although commonly prescribed, acid suppression therapies have no proven benefit in BRUE because most reflux events are not acidic and do not correlate with BRUE episodes[20][40][41].
Best practice point 12: Offer safe sleep education and cardiopulmonary resuscitation (CPR) resources (i.e., community courses) as public health measures for all caregivers, not because BRUE increases risk.
For many concerned families, learning CPR can provide a valuable sense of preparedness and control[1][42].
Best practice point 13: Do not routinely recommend home cardiorespiratory monitoring for otherwise healthy infants following BRUE. Routine home monitoring has shown no benefit in preventing sudden infant death syndrome (SIDS), may trigger false alarms, and cause anxiety[1][43].
Future directions
Further research should clarify effective strategies for communicating BRUE-associated risks and diagnostic uncertainty to families. While routine broad testing is discouraged, studies should define targeted testing and monitoring approaches for infants with risk factors, especially recurrent events. Also, evaluating the benefit and optimal timing of follow-up is needed to improve outpatient recommendations. Finally, research is needed to identify safe methods to reduce unnecessary resource utilization and implement recommendations effectively.
Figure 3. Recommendations for clinical management of infants with suspected BRUE
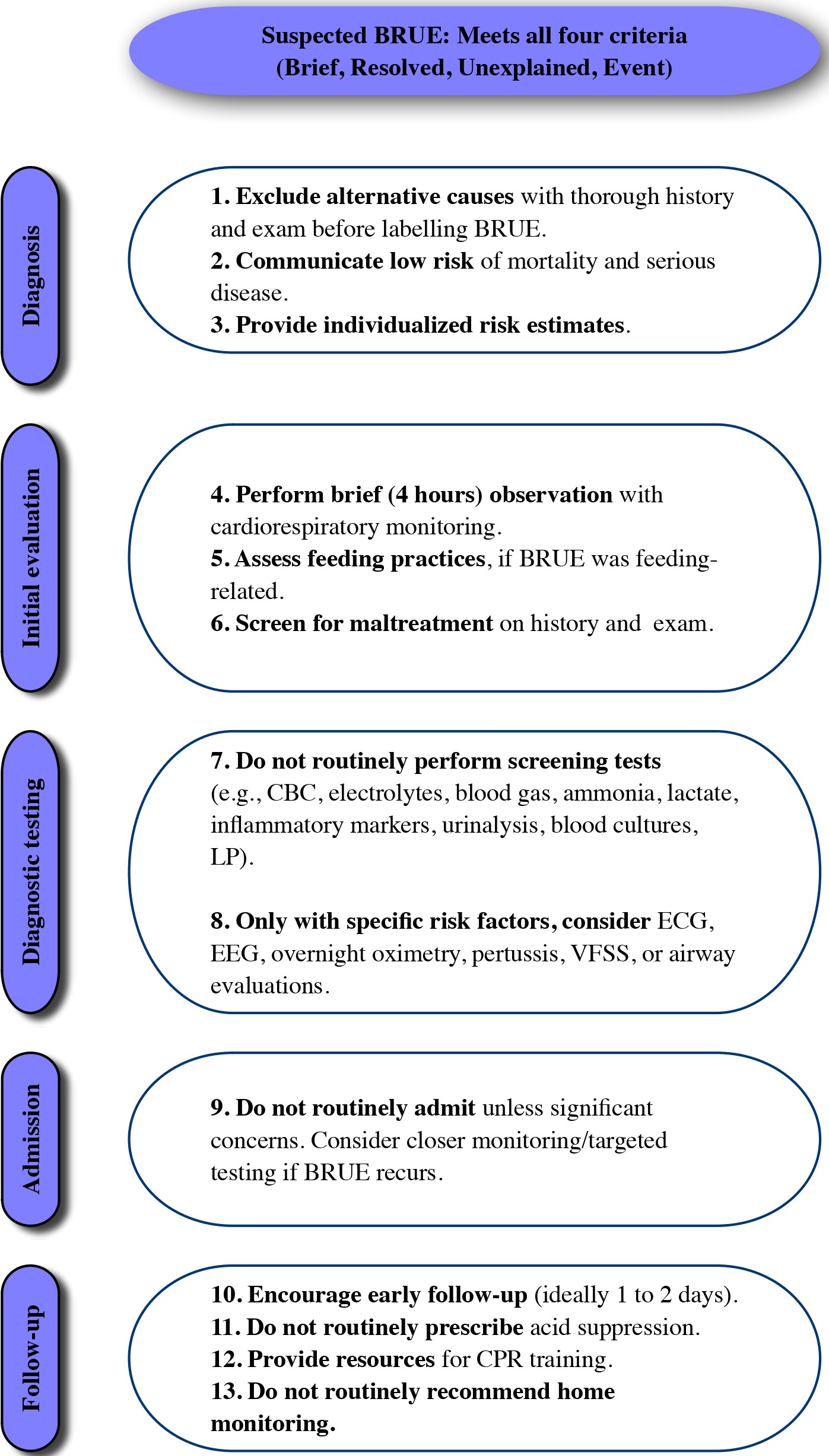
CPR, cardiopulmonary resuscitation; ECG, electrocardiogram; EEG, electroencephalogram; GER, gastroesophageal reflux; GERD, gastroesophageal reflux disease LP, lumbar puncture; VFSS, videofluoroscopic swallow study.
Acknowledgement
This practice point was reviewed by the Acute Care and Community Paediatrics Committees and the Paediatric Emergency Medicine Section Executive of the Canadian Paediatric Society.
CANADIAN PAEDIATRIC SOCIETY HOSPITAL PAEDIATRICS SECTION EXECUTIVE (2025-2026)
Members: Sepideh Taheri MD (President), Laura Davies MD (President-Elect), Melanie Buba MD (Past President), Geert 't Jong MD PhD (Secretary-Treasurer), Peter J. Gill MD DPhil MSc (Member at Large), Jennifer Lee Wiebe MD (Member at Large)
Principal authors: Nassr Nama MD MSc, Kara Picco MD, Olivia Ostrow MD, Joel S. Tieder MD MPH, Peter J. Gill MD DPhil MSc
Funding
There is no funding to declare.
Potential Conflict of Interest
Olivia Ostrow reported receiving an annual stipend as the Pediatrics lead for Choosing Wisely Canada. Joel Tieder reported receiving honoraria from the Children’s Hospital Association as a research consultant for DEI reports. No other disclosures were reported.
References
- Tieder JS, Bonkowsky JL, Etzel RA, et al; American Academy of Pediatrics, Subcommittee on Apparent Life-Threatening Events. Brief resolved unexplained events (formerly apparent life-threatening events) and evaluation of lower-risk infants. Pediatrics 2016;137(5):e20160590. doi: 10.1542/peds.2016-0590
- Merritt JL, Quinonez RA, Bonkowsky JL, et al. A framework for evaluation of the higher-risk infant after a brief resolved unexplained event. Pediatrics 2019;144(2):e20184101 doi: 10.1542/peds.2018-4101
- Nama N, DeLaroche A, Bonkowsky JL, Gremse D, Tieder JS. Brief resolved unexplained event: Evidence-based and family-centered management. Pediatr Rev 2024;45(10):560–72. doi: 10.1542/pir.2024-006351
- Nama N, Liebert S, Abaji M, et al. Infant outcomes, risk factors, and diagnostic yield after a brief resolved unexplained event: A systematic review and meta-analysis. JAMA Pediatr 2026;180(3):250-62. doi: 10.1001/jamapediatrics.2025.5858
- Bochner R, Tieder JS, Sullivan E, et al; Brief Resolved Unexplained Event Research and Quality Improvement Network. Explanatory diagnoses following hospitalization for a brief resolved unexplained event. Pediatrics 2021;148(5):e2021052673. doi: 10.1542/peds.2021-052673
- Nama N, Lee Z, Picco K, et al; Canadian BRUE Collaboration (C-BRUE-C) and the Canadian Paediatric Inpatient Research Network (PIRN). Identifying serious underlying diagnoses among patients with brief resolved unexplained events (BRUEs): A Canadian cohort study. BMJ Paediatr Open 8(1):e002525. doi: 10.1136/bmjpo-2024-002525
- Tieder JS, Sullivan E, Stephans A, et al; Brief Resolved Unexplained Event Research and Quality Improvement Network. Risk factors and outcomes after a brief resolved unexplained event: A multicenter study. Pediatrics 2021;148(1):e2020036095. doi: 10.1542/peds.2020-036095
- Correa CV, Osorio KP, Riffo CA, Luchinni VW. Patients with diagnosis of “BRUE” treated in Chilean pediatric hospital. Applying new terminology. Rev Chil Psiquiatr Neurol Infanc Adolesc 2021;32(2):22–37.
- Nama N, Hall M, Neuman M, et al; Brief Resolved Unexplained Event Research and Quality Improvement Network. Risk prediction after a brief resolved unexplained event. Hosp Pediatr 2022;12(9):772–85. doi: 10.1542/hpeds.2022-006637
- Denis M, Brulé C, Lauzier B, Brossier D, Porcheret F. Brief resolved unexplained event: Severity-associated factors at admission in the pediatric emergency ward. Arch Pédiatrie 2023;30(6):389–95. doi: 10.1016/j.arcped.2023.05.005
- Ramgopal S, Soung J, Pitetti RD. Brief resolved unexplained events: Analysis of an apparent life threatening event database. Acad Pediatr 2019;19(8):963–8. doi: 10.1016/j.acap.2019.08.001
- Nama N, Shen Y, Bone JN, et al; Canadian BRUE Collaboration (C-BRUE-C) and the Canadian Paediatric Inpatient Research Network (PIRN). External validation of brief resolved unexplained events prediction rules for serious underlying diagnosis. JAMA Pediatr 2024;179(2):188-96. doi: 10.1001/jamapediatrics.2024.4399
- Nama N, Hosseini P, Lee Z, et al; Canadian Paediatric Inpatient Research Network (PIRN). Canadian infants presenting with brief resolved unexplained events (BRUEs) and validation of clinical prediction rules for risk stratification: A protocol for a multicentre, retrospective cohort study. BMJ Open 2022;12(10):e063183. doi: 10.1136/bmjopen-2022-063183
- DeLaroche AM, Nama N, Tieder JS. Acute care management of brief resolved unexplained events. Pediatr Emerg Care 2024;41(3):245–50. doi: 10.1097/pec.0000000000003277
- Chevalier I, Beck CE, Doré-Bergeron M-J, Orkin J. Medical management of gastro-esophageal reflux in healthy infants. Paediatr Child Health 2022;27(8):503–11. doi: 10.1093/pch/pxac068
- Duncan DR, Golden C, Larson K, Growdon AS, Liu E. A prospective study of diagnostic testing and hospital charges after brief resolved unexplained event. J Pediatr Gastroenterol Nutr 2025;80(4):623-32. doi: 10.1002/jpn3.12465
- Ward MGK, Ornstein A, Niec A, Murray CL; Canadian Paediatric Society, Child and Youth Maltreatment Section. The medical assessment of bruising in suspected child maltreatment cases: A clinical perspective. Paediatr Child Health 2013;18(8):433-7.
- Chauvin-Kimoff L, Allard-Dansereau C, Colbourne M. The medical assessment of fractures in suspected child maltreatment: Infants and young children with skeletal injury. Paediatr Child Health 2018;23(2):156–60. doi: 10.1093/pch/pxx131
- Doswell A, Anderst J, Tieder JS, et al; Brief Resolved Unexplained Event Research and Quality Improvement Network. Diagnostic testing for and detection of physical abuse in infants with brief resolved unexplained events. Child Abus Negl 2023;135:105952. doi: 10.1016/j.chiabu.2022.105952
- Duncan DR, Growdon AS, Liu E, et al. The impact of the American Academy of Pediatrics brief resolved unexplained event guidelines on gastrointestinal testing and prescribing practices. J Pediatr 2019;211:112-19.e4. doi: 10.1016/j.jpeds.2019.04.007
- Lirette M-P, Wright N, Trottier ED, Beck CE. Management of febrile neutropenia in immunocompetent children and youth. Paediatr Child Health 2023;28(5):324–30. doi: 10.1093/pch/pxac127
- Mittal MK, Tieder JS, Westphal K, et al. Diagnostic testing for evaluation of brief resolved unexplained events. Acad Emerg Med 2023;30(6):662–70. doi: 10.1111/acem.14666
- Nama N, Picco K, Kyrychenko P, et al; Canadian BRUE Collaboration (C-BRUE-C), Canadian Paediatric Inpatient Research Network (PIRN). Interhospital variation in the management of brief resolved unexplained events (BRUE) in infants: A Canadian multicenter cohort study. J Hosp Med 2025;20(12):1297-1305. doi: 10.1002/jhm.70094
- Nama N, Rajasegaran PJ, McDaniel LM, et al; Canadian BRUE Collaboration (C-BRUE-C), Canadian Paediatric Inpatient Research Network (PIRN). Specialty consultations and diagnostic testing accuracy after brief resolved unexplained events: A multicenter observational study. Hosp Pediatr 2025;15(7):563-72. doi: 10.1542/hpeds.2024-008305
- Khan A, Wallace SS, Sampayo EM, Falco C. Caregivers’ perceptions and hospital experience after a brief resolved unexplained event: A qualitative study. Hosp Pediatr 2019;9(7):508–15. doi: 10.1542/hpeds.2018-0220
- Brand DA, Mock A, Cohn E, Krilov LR. Implementing the 2016 American Academy of Pediatrics guideline on brief resolved unexplained events. Pediatr Emerg Care 2021;37(5):e243–8. doi: 10.1097/pec.0000000000001659
- Nama N, DeLaroche AM, Gremse DA. Brief resolved unexplained event (BRUE): Is reassurance enough for caregivers? Hosp Pediatr 2022;12(12):e440–2. doi: 10.1542/hpeds.2022-006939
- Duncan DR, Liu E, Growdon AS, Larson K, Rosen RL. A prospective study of brief resolved unexplained events: Risk factors for persistent symptoms. Hosp Pediatr 2022;12(12):1030–43. doi: 10.1542/hpeds.2022-006550
- Serin HM, Şimsek E, Köroğlu ÖA, et al. Necessity of electroencephalography in high-risk brief resolved unexplained event. J Pediatr Res 2019;6(4):336–41. doi: 10.4274/jpr.galenos.2019.80958
- Morin-Gagnon R, Gagnon J-A .126 BRUE and evaluation of higher-risk infants with overnight oximetry. Paediatr Child Health 2021;26(Suppl 1):e89–e90. doi: 10.1093/pch/pxab061.101
- DeLaroche AM, Haddad R, Farooqi A, Sapién RE, Tieder JS. Outcome prediction of higher-risk brief resolved unexplained events. Hosp Pediatr 2020;10(4):303–10. doi: 10.1542/hpeds.2019-0195
- Sethi A, Baxi K, Cheng D, Laffey S, Hartman N, Heller K. Impact of guidelines regarding brief resolved unexplained events on care of patients in a pediatric emergency department. Pediatr Emerg Care 2021;37(12):e1468–72. doi: 10.1097/pec.0000000000002081
- Giadach C, Mesa T, Abara S, Nalegach ME, Castillo A. Análisis de causas atribuidas a “BRUE” entre los años 2017 a 2020. Rev Chil Psiquiatr Neurol Infanc Adolesc 2022;33(3):36–47.
- Vigne MH, Moreau M, Gascoin G, Darviot E. Descriptive analysis of infant population younger than 1 year admitted for BRUE. Arch Pediatr 2023;30(5):271–6. doi: 10.1016/j.arcped.2023.02.006
- Jarasvaraparn C, Gallegos MBR, Mulekar MS, Wang B, Gremse DA, Crissinger KD. Short article: The endoscopic and histologic findings of infants who have experienced brief resolved unexplained events. Eur J Gastroenterol Hepatol 2018;30(2):195–200. doi: 10.1097/meg.0000000000001012
- Patra KP, Hall M, DeLaroche AM, Tieder JS. Impact of the AAP guideline on management of brief resolved unexplained events. Hosp Pediatr 2022;12(9):780–91. doi: 10.1542/hpeds.2021-006427
- Hochreiter D, Sullivan E, DeLaroche AM, et al; Brief Resolved Unexplained Event Research and Quality Improvement Network. Learning from a national quality improvement collaborative for brief resolved unexplained events. Pediatrics 2024;153(2):e2022060909. doi: 10.1542/peds.2022-060909
- Nama N, DeLaroche AM, Neuman MI, et al. Epidemiology of brief resolved unexplained events and impact of clinical practice guidelines in general and pediatric emergency departments. Acad Emerg Med 2024;31(7):667–74. doi: 10.1111/acem.14881
- Maksimowski K, Haddad R, DeLaroche AM. Pediatrician perspectives on brief resolved unexplained events. Hosp Pediatr 2021;11(9):996–1003. doi: 10.1542/hpeds.2021-005805
- Jarasvaraparn C, Gallegos MBR, Wang B, Crissinger KD, Gremse DA. The characteristics of esophageal multichannel intraluminal impedance-ph measurements in infants experiencing brief resolved unexplained events. Ann Gastroenterol Dig Disord 2018;1(1):1–8.
- Berry JG, Mansbach JM. Questionable safety of proton pump inhibitor use in children. JAMA Pediatr 2023;177(10):1010–2. doi: 10.1001/jamapediatrics.2023.2906
- Knapp J, Pyles LA; AAP Committee on Pediatric Emergency Medicine. Role of pediatricians in advocating life support training courses for parents and the public. Pediatrics 2004;114(6):1676. doi: 10.1542/peds.2004-2020
- Sodini C, Paglialonga L, Antoniol G, Perrone S, Principi N, Esposito S. Home cardiorespiratory monitoring in infants at risk for sudden infant death syndrome (SIDS), apparent life-threatening event (ALTE) or brief resolved unexplained event (BRUE). Life (Basel) 2022;12(6):883. doi: 10.3390/life12060883
Disclaimer: The recommendations in this position statement do not indicate an exclusive course of treatment or procedure to be followed. Variations, taking into account individual circumstances, may be appropriate. Internet addresses are current at time of publication.